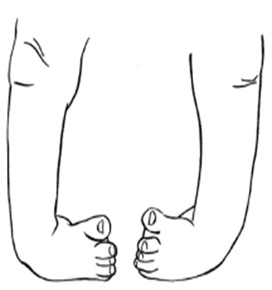
Typical appearance of untreated clubfeet. Courtesy of Shriners Hospital.
Description
Clubfoot is a condition in which the foot is turned and twisted inward. This is present at birth (and in some cases may be detected on prenatal ultrasound). It is one of the most common birth anomalies. Clubfoot is more common in males, and occurs in both feet about half the time.
Babies can have clubfeet as their only problem or clubfeet can happen with other problems that affect the baby’s nerves, muscles or tendons. Clubfeet in babies who have other problems can be stiffer and harder to treat than clubfeet that happen alone. No one knows what causes clubfeet but they tend to be passed along in families.
If treated, most kids will be able to walk, wear shoes and play sports without pain. Most treatment doesn’t require an operation.
Definitions:
Clubfoot brace – Shoes or sandals attached to a bar to prevent recurrence after the clubfoot is corrected. The brace is often also referred to as a “foot abduction orthosis” or the “Ponseti brace”.
Achilles (heel cord) tenotomy – Minimally invasive procedure to lengthen the Achilles tendon. This is frequently required as part of the treatment of clubfoot
Symptoms
Babies with clubfoot are not in pain, but the position of their feet will not correct without a doctor’s treatment. Over time, clubfeet that are not treated will become painful and limit the ability to walk
Examination
In addition to examining your child’s feet, your doctor will perform an overall physical examination to look for other problems. Other testing such as xrays is usually not necessary.
Treatment
The goal of clubfoot treatment is to give the baby a normal foot. It is best to treat babies shortly after birth so the foot is corrected before they start trying to walk. It is possible to treat clubfoot in older children.
Ponseti Casting
The mainstay of clubfoot treatment is Ponseti casting, which is a set of casts that, in series, bring the foot around to a neutral position. Each week, the child’s foot is gently stretched and a cast is placed from the toes to the upper thigh; with each week’s cast, the position improves. This process usually takes about 6 to 8 weeks. At the end of this period, a small procedure to lengthen the tight Achilles tendon is often required. This is done through a very small incision, and another cast is placed afterwards for several weeks. Some practitioners do this in the office, and in some places this is done in the operating room under sedation.
Once this last cast comes off, the foot (or feet) should be in a neutral, corrected position. However, if left alone at this point, there is a high chance of recurrence, so the child’s foot or feet are braced to maintain the correction. Usually this is done with a special brace - shoes attached to a bar. This brace is worn initially 23 hours a day, and then after several months the brace may be worn just at night and at naptime. The brace will usually have to be worn at night for several years.
After treatment it is very important for parents to make sure the baby wears the brace. The biggest reason for the clubfoot position to come back is not wearing the brace. If the clubfoot position does come back – the baby will need to be casted again. The baby might need to have the Achilles tendon lengthened again or additional surgery.
French Method
In some countries, clubfoot is corrected by a physical therapist. The therapist stretches the baby’s foot every day and then uses taping and splinting as progress is made. The parents are taught to do the stretches at home too. It takes longer to get a normal foot position with stretching. The baby may still need to have the Achilles tendon lengthened. These babies wear splints until age 2 or 3.
Surgery
In bad cases of clubfoot, surgery may be needed to correct the foot position. This can involve lengthening or moving tendons. Metal pins can be used to hold the bones in their new position. After surgery – the foot will be in a cast.
Outcomes
Clubfoot does not resolve on its own. With treatment, most clubfeet are correctable and have good function. The affected foot may always be smaller than the other foot, and the calf on the affected side may also always be smaller.
Tips for Success with the Clubfoot Brace
Clubfoot treatment is a long process that can be very frustrating for the parents and the doctor. Here are some helpful tips:
Play in the brace - use the bar to help your child kick and swing his/her legs
Stay in a routine - always wear the brace in the crib
Add padding to the bar
Don’t use lotion under the shoes
Carefully secure straps & buckles
Check the skin at least 3 times per day for signs of a pressure sore
Clubfoot is a condition in which the foot is turned and twisted inward. Some of the muscles connecting the foot to the leg may be short and tight as well.
Q: When does clubfoot happen?
Clubfoot is present at birth, and may be detected on prenatal ultrasound.
Q: Is clubfoot common?
It is present in about one in 1,000 births.
Q: Who gets clubfoot?
Clubfoot is more common in boys, and does seem to have a genetic/familial component. In some cases it is associated with further neuromuscular conditions, such as spina bifida or arthrogryposis.
Q: Will this get better on its own?
No. If left untreated, the child will not be able to walk properly.
Q: How is clubfoot treated?
Clubfoot is usually treated with a series of casts to gradually bring the foot into a neutral position. At the end of the casts, a small incision is usually needed to lengthen the over-tight Achilles tendon. Thereafter, a brace with shoes and a bar must be worn to maintain the foot’s good position.
Q: How long does this treatment take?
The initial casts usually take 6 – 8 weeks, and then the cast after lengthening the Achilles takes another 3-4 weeks. The brace must be worn full time for at least 3 months, and then eventually just at night/for naps for several years.
Q: Is more surgery ever needed?
In some difficult cases, more extensive surgery on the foot may be required. This may involve lengthening or rerouting tendons, or releasing soft tissues in the foot.
Q: Will my child be able to walk, run, and play?
Most children have a good outcome and are able to do participate in all activities.
Q: Will the foot look normal?
The treated foot will be mildly smaller but will have a physical appearance similar to other foot. The calf of the affected leg is also usually smaller than the other side.
Q: Is treatment painful?
There may be mild discomfort initially with the casts, and with the Achilles lengthening, but in general the treatment is not painful.
Q: What if my child doesn’t wear the brace afterwards?
Unfortunately, there is a high chance of recurrence without brace wear. Close adherence to the bracing regimen is suggested.