Overview
Non-ossifying Fibroma (NOF) is the most common bone tumor in kids. It may occur in 35% of all children. It is not cancer. NOF is benign, which means it is just a collection of abnormal cells that stays where it is and does not move to other parts of the body. These fibromas occur more in males than in females, and are usually only found because an X-ray was done of that area for another reason, like pain after falling. Many children with an NOF have no symptoms at all, and most often these benign tumors go away without needing any treatment.
Description
NOFs are made of fibrous tissue. They are yellow to brown in color and often appear in the bones around the knee or ankle. Although a patient may have several NOFs, this is very uncommon without having other conditions present.
We do not know what causes NOFs. Other names for NOFs are: metaphyseal fibrous defects, fibrous cortical defects, non-osteogenic fibromas, or cortical desmoids
NOFs generally do not cause any symptoms. It is rare for an NOF to cause pain or lead to a mass that you can feel. A few patients may have mild pain, especially with activity. This usually is due to a small fracture (break in the bone) that occurs if the NOF is large, which can weaken the bone. If there has been pain in the NOF and no fracture, it is possible that the lesion is not an NOF and is actually something else.
Doctor Examination
Your doctor will talk to you and your child about his or her medical history as well as any symptoms that occurred before the NOF was found on the x-ray. He or she will ask about any history of trauma or a fall, any pain, pain with activities, or pain during the night.
Your doctor will see if there are any bony lumps, and whether those areas are painful. He or she will also check the motion in the joints near the area.
Studies
X-rays are used to look at the bone and the tumor. NOF looks like a small round or oval bubble that appears on the edges of the bone with a thin rim of bone that appears white. (Figure 1)
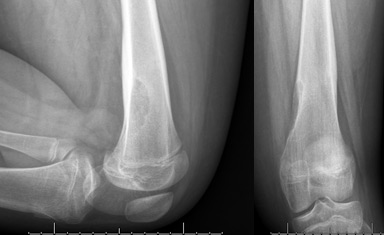
Figure 1 – The NOF is located on the edge of the distal femur (thigh bone). It is a bubbly lesion.
A CT scan or MRI are not always necessary, but may be ordered. (Figure 2) This helps to show exactly how big the NOF is and whether it is causing thinning and weakening of the bone near the NOF. It can also show if there is a fracture (break) through the NOF that is causing the pain.
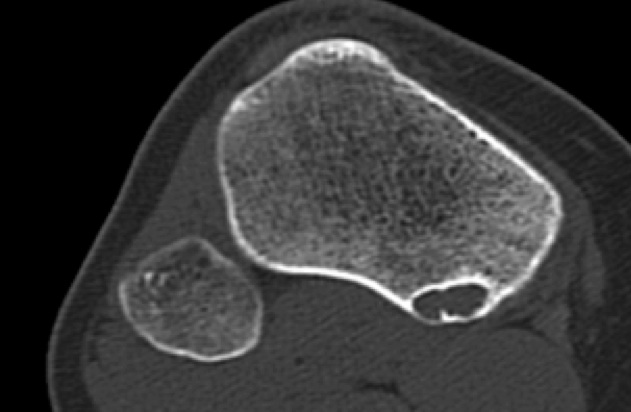
Figure 2– NOF on a CT scan has an appearance of bubbles.
Treatment
The vast majority of NOFs do not require treatment. NOFs will stop growing when you child stops growing, and will gradually fill in with bone.
Your surgeon may recommend surgery, however, if there is a fracture through the NOF, if the NOF is very large and may cause the bone to be weak, or if your child is having pain.
Surgical Treatment
A surgery called curettage involves scraping the tumor out of the bone with special tools. To fill the hole, your surgeon may place bone graft, which can either be bone from your child’s own body, bone from another person, cement, or a bone graft substitute that is made in a lab. Sometimes, your surgeons may also put a chemical in the hole to try to prevent the tumor from coming back. If there is an unstable fracture or if the lesion is very large, your surgeon may recommend placing a plate and screws to stabilize the bone.
Outcome
The chance of the NOF coming back after surgery is very low. These lesions can go away on their own without surgery once children have grown. They do not turn into cancer.
More Information

