Description
Spondylolysis (spon-dee-loh-lie-sis) refers to a fracture, break or defect in one of the bones, called a vertebra, in the lumbar spine (lower back). This is most commonly the fifth (but occasionally the fourth) lumbar vertebra. This is often a stress fracture in the pars region of the vertebrae related to overuse. Spondylolysis is sometimes referred to as a “pars defect”. (Figure 1) In some cases, the defect becomes severe enough for the vertebra to slip out of place. This is called
spondylolisthesis (spon-dee-loh-lis-thee-sis). If the vertebra slips far out of place, there may be pressure on nerves going to the legs. (Figure 2a and 2b).
Some people may be predisposed to these conditions. Certain sports—those which put stress on the bones of the back, especially in hyperextension or bending backwards—are more likely to cause spondylolysis and spondylolisthesis.

Figure 1a &1b - Radiograph of low grade spondylolisthesis of L5-S1 and spondylolysis (pars lucency). Images courtesy of William Phillips, MD, Texas Children’s Hospital, Houston, TX.
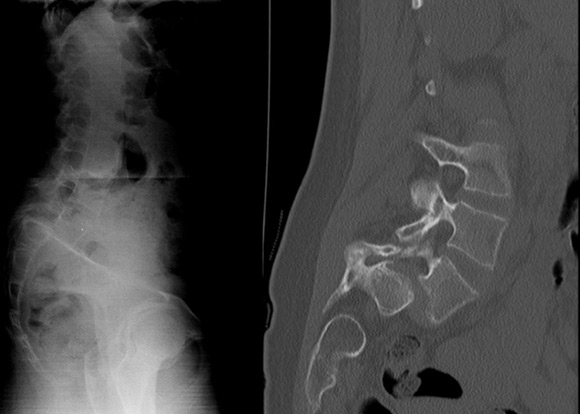
Figure 2a & 2b - X-ray and CT scan images of severe spondylolisthesis. Images courtesy of Pat Cahill, MD, Shriners Hospitals for Children, Philadelphia.
Symptoms
Symptoms may begin with back pain and stiffness, as well as hamstring tightness. Slippage that compresses nerves may cause bowel or bladder problems or pain radiating down the legs. However, not all patients with spondylolysis or spondylolisthesis have pain or other symptoms.
Diagnosis
Your child’s doctor will examine your child’s back, and do a neurological exam to check his/her nerves. X-rays are often used to make the diagnosis, though sometimes other tests such as MRI or bone scan are required.
Treatment
Nonsurgical
Treatment of spondylolysis begins with nonsurgical management. This includes a break from activities, and may also include anti-inflammatory medication, such as ibuprofen. In some cases, physical therapy may be done to stretch and strengthen the muscles of the abdomen and core. Occasionally a brace may be used. Usually these treatments are effective and activities may gradually be resumed. Periodic x-rays are usually also performed to monitor the position of the vertebra.
Surgical
If non-surgical measures are not successful, or if the slip of the bone is severe and/or continues to worsen, surgery may be done to stabilize the vertebra. Often screws and rods are used to hold the vertebra in place. In some situations, a spondylolyis may be repaired and bone grafted. However, the most common surgical procedure for spondylolysis or spondylolisthesis is a fusion of the involved vertebrae. (Figure 3)
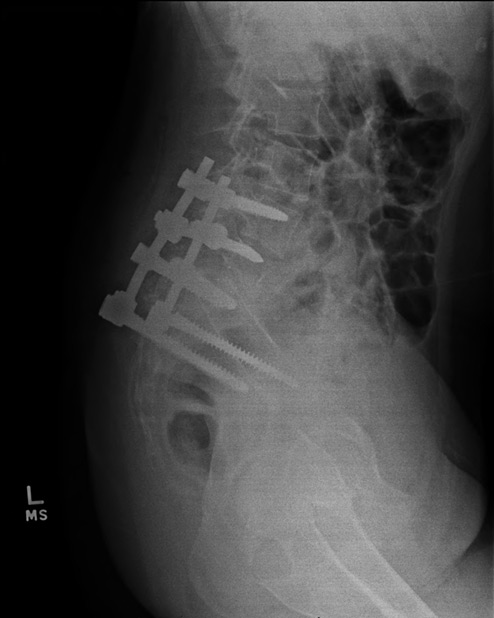
Figure 3 - X-ray of the same patient after surgical fixation. Image courtesy of Pat Cahill, MD, Shriners Hospital for Children, Philadelphia.
More Information

