Hip Fractures (Proximal Femur):
This is a break involving the top part of the femur that makes up part of the hip joint. This kind of fracture can involve the femoral head inside the hip joint, the upper femur growth plate, the femoral neck which connects the head to the rest of the femur bone, or the upper part of the femur shaft.
Femoral Shaft Fractures:
This is a break in the middle part of the femur bone. This information page refers to this type of fracture.
Distal Femur (Knee) Fractures:
This is a break in the lower part of the femur bone, near the knee joint. This kind of fracture can involve the growth plate of the lower end of the femur and may connect to the knee joint.
Stress Fractures:
This is a break that occurs slowly and gradually due to overuse. These injuries may be subtle and sometimes need advanced imaging, like an MRI, for diagnosis.
Open Fractures:
This is a break in the bone that results in the bone being exposed to the outside air through a break in the skin. It is sometimes referred to as a “compound fracture.”
Pathologic Fracture:
This is a break in the bone that happens because of a preexisting problem with the bone, such as a bone cyst or a tumor.
Infants and Toddlers: A fussy child with a swollen, red or crooked thigh/upper leg should be checked for a femur fracture. The child may refuse to use the leg, including not moving it or refusing to walk or crawl. This injury can occur from a low-energy trauma such as the leg being pulled or twisted accidentally, or from a fall while playing, but it can also occur from high-energy trauma such as a car accident. Children with femur fractures should be checked for other injuries. Infants and young children who are not yet able to walk should be evaluated for non-accidental trauma (NAT).
Children and Adolescents: A crooked, swollen, and painful thigh/upper leg should be checked for a femur fracture. Children with this injury may not be able to walk. This injury commonly occurs from low-energy trauma such as sports, but it can also occur from high-energy trauma such as car accident. Children with femur fractures should be checked for other injuries.
Doctors will check the skin and touch different areas of the leg to confirm that the fracture does not extend to the hip or knee. They will check that all the muscles and nerves are working, and that there is good circulation to the rest of the leg and foot.
In most cases, an x-ray will be performed to confirm the diagnosis of a femur fracture. The xrays will include the entire femur, including the knee and hip joints. Other areas of the leg, such as the tibia (lower leg), may be imaged to rule out other injuries or breaks. Your doctor may order additional tests, like a CT scan, if the break is near the joints or growth plates. A CT scan allows your doctor to closely examine the break and helps guide treatment.
Femur fractures are treated based on the age of the child, the location or the fracture, and the alignment of the bone.
Non-surgical:
In very young infants (0-6months), a femur fracture can be treated in a soft harness (Pavlik harness) or in a splint to support the leg while it heals, which takes about 3 weeks.
In toddlers and young children (6 months to 5 years), many femur fractures can be treated in a special type of partial body cast called a spica cast. Most children need to be sedated to set the bone and apply the cast, and this is often done in the operating room. Follow up will be needed to monitor the bone healing. The amount of time in the cast can be up to 6 weeks, but that depends on the age of the child and how the bone is healing. Your doctor may adjust the cast during the healing process. Your child may not be allowed to put any weight on the leg for the first few weeks. Once the bone is healed enough on xrays, your doctor may allow your child to start using the leg for walking again.
For more information on spica cast care, please click on the link: http://orthokids.org/Treatments-Surgery/Spica-Casts
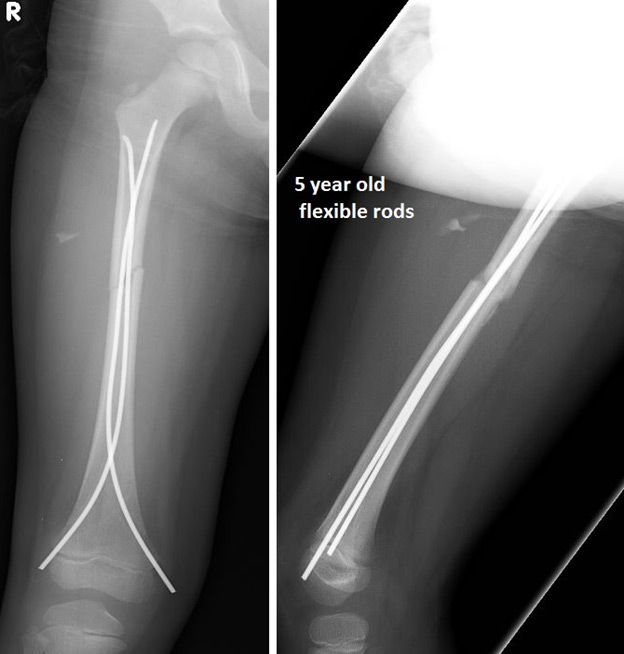
Surgical: Surgery to stabilize the femur bone is more common than casting in school-age children and teenagers. Surgery may be needed in younger children if the bone cannot be lined up properly, or if there is a break in the skin that exposed the bone to the air at the time of the injury. Depending on the type of fracture and the age of the child, your surgeon may use metal pins, a plate and screws, flexible nails, or a rigid nail to fix the femur (see images below). In cases with severe damage to the skin and muscle, an external device (external fixator) may be attached to the femur with pins to hold the bone in place temporarily or until it is fully healed. After surgery, your surgeon will decide when your child can use the leg for any weight-bearing or walking based on the healing of the bone.
Figures: (a) Spica Casts, (b) Plate and Screws, (c) Flexible Nails, (d) Rigid Nail
(a) 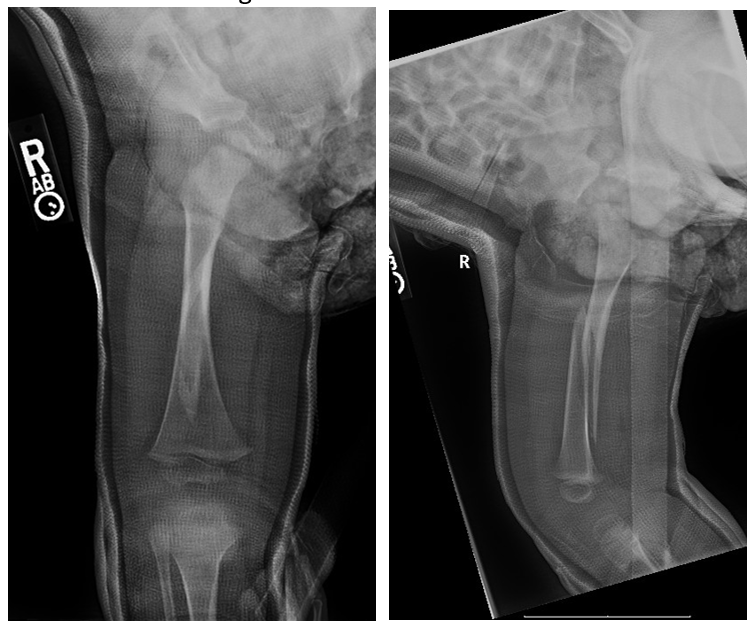
(b) 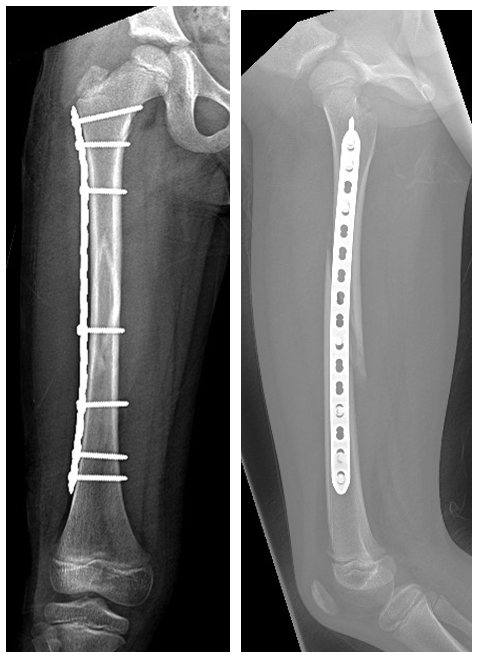
(c) 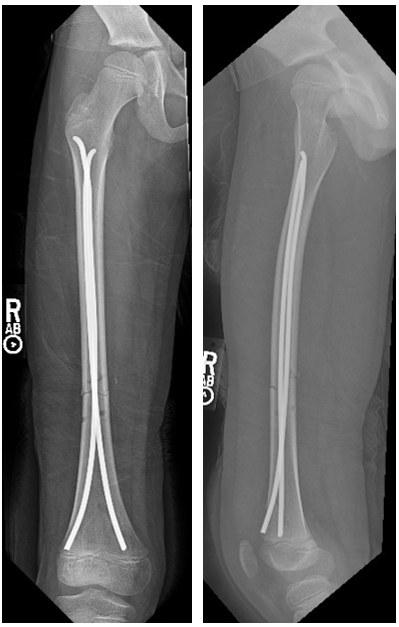
(d) 
In older children and adolescents, surgery is chosen to align the bone with metal implants. Different types of implants may be used in surgery to keep the bones aligned. This may include flexible nails (rods), rigid nails (rods) or even plates and screws. Children and teenagers who are still growing should not get the same rods that adults would get. The placement of adult rods can risk damaging the blood supply to the top of the femur bone and cause long-term problems with the hip joint.
After surgery, a cast or splint may still be used to protect the bones in place during healing.
Figures: 5 year old children with a femur fracture treated with flexible rods (a) after initial surgery (b) healing at 8 weeks; (c) complete healing at 5 months.
(a)
(b) 
(c) 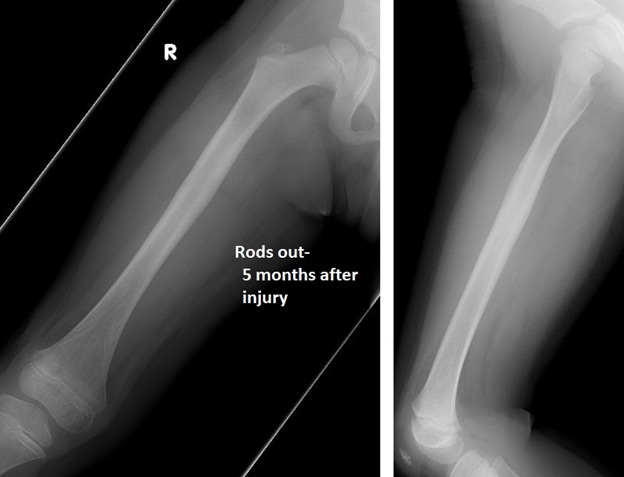
Most children recover from their femur fractures within a few months. They may temporarily limp or have trouble running and jumping due to weakness until they fully recover. Fractures that are treated in a cast may not heal completely straight. Some angulation and a small amount of shortening of the bone (up to 2cm) is acceptable, and this will straighten out and correct over time as your child grows. The vast majority of children who fracture their femur will return to their original level of activity after the fracture has healed. Physical therapy may or may not be required after femur fracture.
In some cases, the doctor may monitor you child over a few years to make sure the bone grows properly. If your child was treated with an implant, your doctor may recommend removing this in the future.
Children are not little adults, but like adults, they need expert care. A pediatric orthopedic surgeon should typically manage these injuries in children in order to make the sure the fracture is adequately aligned, to decrease the risk of complications, and increase the likelihood of a good outcome.

