Overview
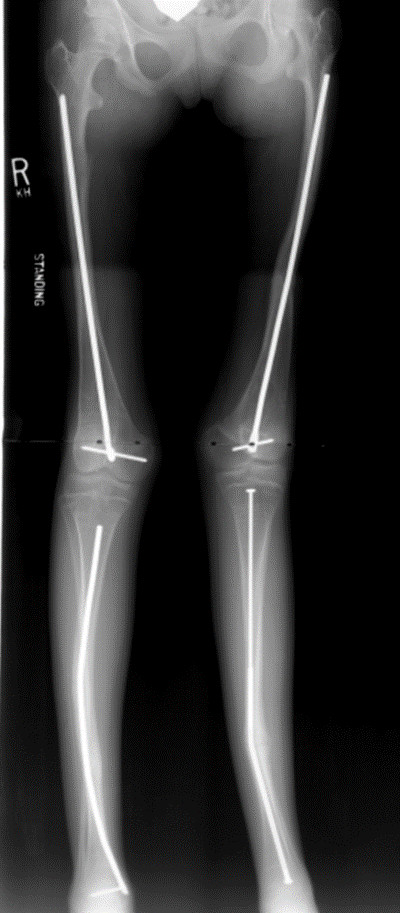
Xray of the lower extremity of a patient with OI who has undergone surgery with telescoping rods.
Osteogenesis Imperfecta (OI) is a rare genetic disorder that causes fragile bones. Osteogenesis Imperfecta means “imperfectly formed bone.” OI is very different from child to child, depending on the severity of the disease in that particular child. Children with a mild form of OI may live for many years with very few fractures (breaks in the bone). Those with severe OI may have hundreds of fractures in their bones.
Cause
Collagen is major part of connective tissue in your body. Type I Collagen helps to make ligaments, bones, skin, and teeth. Children who have OI have a problem in one of their genes that makes Type I Collagen. Their bodies may not be able to make enough collagen, or the collagen that is made is not good quality. This leads to fragile bones that break very easily. However, these bones still heal at a normal rate. Bones that fracture many times may end up being bowed and crooked.
OI is often inherited through a defective gene from one of the parents. However, a child may have a very different form of OI than the parent. There are cases where neither parent has OI, and the child’s gene has spontaneously changed and now does not work properly.
Symptoms
In addition to the abnormal bones, patients with OI may also have blue sclera (the part of the eye that is usually white), crooked bones, scoliosis (curved spine), hearing loss, short height, breathing problems, and bad teeth. Again, symptoms are varied, depending on the type of OI.
There are 4 main types of OI:
Type I – This is the most common form of OI and the mildest type. There is very little bone deformity, but the bones are still easily fractured. The sclera of the eyes have a blue, purple, or gray tint. Hearing loss occurs early. Teeth may get cavities easily or crack.
Type II – This is the most severe form of OI, and many babies often do not survive. Bones may fracture even when the baby is in the womb.
Type III – Babies with this type of OI are often born with fractures, and their bones are very easily broken. The bones become bowed and deformed from multiple fractures. The sclera of the eyes may be white or have a blue, purple, or gray tint. Children are shorter than average, and they may have scoliosis (curved spine), breathing problems, and bad teeth.
Type IV – This OI is moderately severe, between Type I and Type III. Bone deformities are mild to average. Children may have blue sclera that gets whiter when they get older. They may also have bad teeth.
Examination
Bones that break with very little force are the first sign that will lead your doctor to suspect OI. He or she will ask about family’s medical history as well as your child’s medical history and history of broken bones. Your doctor will carefully examine your child’s skin, bone alignment, hair, teeth, and eyes.
Other Tests
X-rays are used to diagnose fractures as well as look at the crookedness of the bones.
Blood tests or skin tests may be needed to make the diagnosis. These tests are used to look for the genes that are defective in OI.
Ultrasound during pregnancy may detect severe OI.
Treatment
There is no cure for OI. However, there are treatments can help with the strength of the bone and can help when your child has a fracture.
Medication – though it is still experimental, sometimes medicine called bisphosphonates can be used to make the bone stronger and less likely to have fractures. They also help with bone pain. They can be given by mouth or through an IV that delivers the medicine into the blood.
Casts/splints – casts and splints are used to hold a broken bone in place while it heals.
Orthoses – lightweight plastic and metal braces can be used on the legs to help patients with severe OI to walk.
Exercise – low impact, weight bearing exercises can help to strengthen the bone, especially after a fracture. The body’s motto is “use it or lose it”– the more you use the bones and muscles for exercise or walking, the stronger the bones and muscles become.
Surgery – your doctor may recommend surgery if a bone breaks several times in the same place or the bone does not heal in a straight position after a fracture. Most of the time, the bones are fixed with straight rods that go down the middle of the bone (like a stick placed in the middle of a straw). Some rods will grow with your child, while others may need to be replaced as your child grows.
Children with severe curvature of the spine (scoliosis) may also need surgery to help straighten the back. Scoliosis bracing does not work well in patients with OI because the ribs are too fragile for the pressure of the brace.
Outcomes
For many children with OI, the number of bone fractures tends to diminish later in life. Adults should avoid medications that decrease bone density, such as steroids, if possible. Smoking and drinking may also lower bone density. Fractures may become more frequent again after menopause in women and beyond age 60 in men.

Femur xray with a healing break around a telescoping rod.
References

