Description
The forearm has 2 bones – one is called the radius (on the same side of the forearm as the thumb) and the other is the ulna (on the same side of the forearm as the small finger). Forearm fractures can occur anywhere in these bones, from the elbow to the wrist, and may even be associated with a dislocation (when a bone pops out of a joint). Forearm fractures often occur through the growth plate, which is made of cartilage, because the cartilage is weaker than the bone.
Children love to play and run, and this can lead to a child falling onto their arm, leading to a fracture. Forearm fractures are the most common fractures in children (up to 50% of all fractures in children!) and occur in 1 out of every 100 children. The vast majority of these fractures can be treated with just a cast or splint, although some of them may need to be reset to improve the alignment of the bones.
Types of fractures
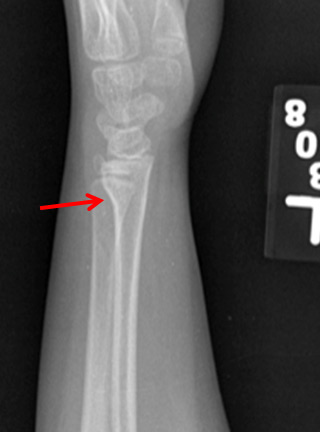
Physeal (Growth Plate) fracture:
This occurs when the growth plate or physis through the wrist is involved in the injury. These fractures are especially common near the wrist. There is a large amount of remodeling potential when fractures occur near or through physis, especially in younger children.

X-ray example of a growth plate fracture (red arrow) at the wrist.
This occurs when only one side of the bone is compressed and buckles but does not break all the way through. This is like when you push down on an empty paper towel roll and the roll buckles but does not break. The other side of the same bone is not affected.

X-ray example of a torus or buckle fracture (red arrows) of the wrist (AP).
X-ray example of a torus or buckle fracture (red arrows) of the wrist (Lateral)
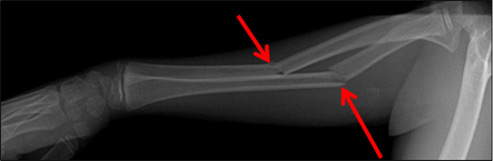
Greenstick fracture:
This occurs when one side of the bone breaks but the other side of the bone is simply bent (red arrows). This is occurs because children’s bones are still very soft compared to adult bones.
 Plastic deformation fractures:
Plastic deformation fractures:
This occurs when the bones bend but do not break. Many times you cannot see a break on the x-ray but the bones may look bowed. Again, this occurs in children only because their bones are still very soft.

X-ray example of plastic deformation. The bones in the forearm are bowed but not broken.
Complete fractures:
This is when the bones are completely separated and not touching on the x-ray.


X-ray example of complete fractures of the radius and ulna
Monteggia fractures:
This occurs when the ulna has a fracture and the radial head (the part of the radius near the elbow) has dislocated from the elbow joint.

X-ray example of Monteggia fracture. The ulna is broken and the radial head is dislocated at the elbow (red arrow)
Figure: X-ray example of Monteggia fracture. The ulna is broken and the radial head is dislocated at the elbow (red arrow).
Galeazzi fracture:
This injury involves a fracture of the radius and the ulna is dislocated at the wrist.

In a Galeazzi fracture-dislocation, the radius is fractured (red arrow), and the wrist is dislocated (red circle).
Symptoms
A crooked arm, swelling, pain, an inability to move the arm, and bruising are the most obvious signs that there is a fracture. In severe injuries, the skin near the bone may have an open wound with bleeding. If that happens, this is an emergency, and you should bring your child to the emergency room to prevent the bone from getting infected. Severe injuries may also be accompanied by numbness and tingling in the hand or forearm. You should bring your child to the emergency room if that happens. Pain that does not get better on its own may also be a sign of a fracture, even if the arm does not look crooked.
Examination
The doctor will carefully look at the skin around the elbow, forearm, and wrist as well as touch those areas to see what hurts. He or she may also try to gently move the joints. Testing the nerves and circulation to the hand are also important.
Other Tests
Most of the time, simple x-rays are all that are needed to diagnose a forearm fracture. Because forearm fractures can be associated with fractures of the wrist and elbow, your doctor will usually obtain x-rays of those areas as well.
Treatment
The vast majority of forearm fractures can be treated without surgery. Stable fractures such as a buckle or torus fracture can generally be treated in a splint or cast for 3 to 4 weeks. If the bones are angled, the doctor may need to reset the bones to get a better alignment and then put a cast on to hold the bones in place while they heal. Depending on how great the deformity is, this manipulation may occur in the clinic, under sedation in the emergency room, or even in the operating room. In young children, some angulation and displacement is often acceptable because of rapid healing and reliable remodeling. Many times your child will need to come back for a repeat x-ray in 7 to 10 days to make sure that the bones stay in a good position. Most forearm fractures require a cast for at least 6 weeks, and sometimes even for 12 weeks depending on the severity of the fracture and how well it is healing. Sometimes at the 6 week mark, the long arm cast can be changed to a shorter cast.
Surgical Treatment
Surgery may be needed in some circumstances:
- There is a cut in the skin near the broken bone
- The bones will not stay lined up even in a cast
- The bones have started to heal in a bad position and cannot be manipulated because of the healing.
- The injury is closer to the elbow and the bones are not well aligned
Different types of implants may be used in surgery to keep the bones aligned. This may include temporary pins or plates and screws. After surgery, a cast or splint may still be used to help keep the bones in place during healing.
Outcomes
Fractures near wrist generally have rapid healing and injuries near middle of forearm may take longer to heal and have higher chance of re-fracture. Stiffness in the elbow and/or wrist is common after coming out of the cast or splint. This usually gets better on its own after a few weeks, but in rare cases, physical therapy is needed to help regain motion. Because the bones are still weak after getting out of the cast, your doctor may recommend that your child avoids sports and physical education for 4 to 6 weeks afterwards to prevent the bone from re-breaking if your child falls onto the arm. If the fracture involves the growth plate, your doctor may want to repeat the radiograph in 6 to 12 months to make sure the bone is still growing normally.
More Information






